Healthcare providers in the United States face increasing pressure to transition to value-based care models, where compensation is linked to patient health outcomes rather than the volume of services provided. The financial benefits are evident: value-based care helps providers cut unnecessary costs while earning incentives for delivering high-quality, efficient care. These payments come from government programs like Medicare and Medicaid or private insurers.
To make value-based care models successful, reliable and up-to-date data is essential. Healthcare organizations must prove that reducing the number of procedures and tests does not compromise patient outcomes. This requires a greater emphasis on preventive care, such as offering programs for patients at risk of chronic conditions like heart disease or diabetes. Additionally, organizations must invest in technology capable of gathering, analyzing, and presenting data to demonstrate how care improvements affect patient health and experience.
In this blog, we will thoroughly explain value-based care, exploring its key variables, challenges, and benefits, while also highlighting how MedCare MSO can assist in ensuring a smooth transition to this model.
Schedule a free consultation to improve patient outcomes
What Is Value-Based Care?
Value-based care refers to healthcare delivery models that prioritize improving patient outcomes while managing healthcare costs. In this model, healthcare providers are compensated based on the results they achieve rather than the number of services they provide. This shift incentivizes providers to focus on the quality of care, performance, and patient satisfaction.
Value-based care applies to both patients covered by government programs like Medicaid, Medicare, and the Veterans Health Administration, as well as those receiving private healthcare. With its extensive experience in developing and overseeing value-based care initiatives, the Centers for Medicare & Medicaid Services (CMS) is in a prime position to lead the charge in creating a unified approach to value-based care across the entire healthcare system.
CMS can also play a role in encouraging hesitant providers to adopt these models. To accelerate adoption, it may become necessary to make participation in value-based care programs mandatory.
Value-Based Care Models vs. Fee-for-Service Models
| Fee-for-service care | Value-based care |
| Financial rewards for clinicians to perform more procedures or treatments | Financial rewards tied to the quality of care |
| Providers paid for all procedures, regardless of necessity | Providers paid for improving patient health outcomes |
| Fragmented care where providers can’t see the full patient history | Collaborative approach where providers work together to prevent unnecessary tests and procedures |
| Reimbursement remains unchanged, no matter the patient’s outcomes | Emphasis on wellness and prevention to reduce the need for expensive treatments in the future |
Fee-for-service models reward providers based on the number of treatments and tests given, encouraging more procedures, like additional tests or extended hospital stays. In contrast, value-based care focuses on efficiency and cost reduction, compensating providers for the quality of care they deliver. For instance, the UK’s RightCare program offers a toolkit to help local health providers speed up diagnoses, treatments, and access to specialists for patients with neurological conditions.
Goals for Medicare Value-Based Payment Programs
| Hospital inpatient care | Ambulatory care | Health plans | Post-acute care |
| Reducing readmissions, decreasing infection rates, and improving communication | Enhanced patient satisfaction, cost-efficiency, and physician performance | High-quality scores that qualify for bonus incentives | Improved patient ability to perform daily activities, better cognitive function, and reduced fall risk |
Medicare value-based payment programs aim to address a major issue in U.S. healthcare: despite higher spending compared to other countries, the outcomes are not as strong. These programs are divided into four main categories: inpatient care, outpatient care, health plan initiatives, and post-acute care.
Top 8 Variables in the Value-Based Care Model
Accountable Care Organizations (ACO)
Accountable Care Organizations (ACOs) are groups of healthcare providers, including doctors, hospitals, and specialists, that collaborate to deliver coordinated care to patients. The focus of an ACO is on ensuring that patients receive the right care at the right time, avoiding unnecessary tests, procedures, and hospitalizations. This model encourages the provision of high-quality care while keeping costs in check.
Mechanism:
ACO participants are responsible for managing the health of a specific patient population. These organizations receive payments tied to both improvements in care quality and reductions in healthcare costs. For example, under Medicare, ACO participants can earn shared savings if they lower overall spending while maintaining or improving care outcomes. Conversely, they may face penalties if they fail to meet quality and cost benchmarks.
Key Benefits:
- Coordination: ACOs encourage healthcare providers to work together, reducing fragmentation and improving patient outcomes.
- Cost efficiency: Providers benefit from reducing unnecessary care and hospital visits, which in turn reduces overall healthcare spending.
- Improved care: ACOs focus on preventive care and managing chronic conditions, which can lead to better long-term health for patients.
Bundled Payments
Bundled payment programs provide a single, fixed payment to cover all services related to a particular treatment or procedure. This approach consolidates payments for different healthcare services, including pre-operative, surgery, and post-operative care, into one lump sum. The responsibility for managing the care and costs of the patient’s treatment lies with a single provider, called the “awardee,” who works with other providers involved in the care.
Mechanism:
Under the CMS’s Bundled Payments for Care Improvement initiative, healthcare organizations take financial and performance responsibility for a patient’s entire course of care. This includes working with other providers to ensure that all aspects of care are delivered efficiently. However, there are concerns about the potential for fragmented care, as coordinating services across multiple providers and settings can be challenging.
Key Benefits:
- Cost control: Providers have a strong incentive to eliminate unnecessary tests, procedures, and treatments to stay within the fixed payment amount.
- Comprehensive care: Providers are incentivized to deliver the full range of care needed for the patient’s condition, ensuring better outcomes.
- Coordination challenge: While bundled payments can drive efficiency, the model requires careful coordination to avoid fragmentation of care across providers.
Patient-Centered Medical Homes (PCMH)
The Patient-Centered Medical Home (PCMH) model is centered around enhancing the primary care experience. The goal is to coordinate all care across providers to ensure that patients receive timely and efficient services. Unlike traditional primary care, which may be more fragmented, PCMH emphasizes accessibility, continuity, and comprehensive care management.
Mechanism:
PCMH operates by organizing a team of healthcare providers, including primary care physicians and specialists, to work together and coordinate care across different settings, such as specialist offices and hospitals. Providers in the PCMH model ensure patients have access to their care team through extended office hours, digital communication, and after-hours support. The model emphasizes preventive care and chronic disease management, helping to improve overall health outcomes and reduce the need for emergency visits or hospitalizations.
Key Benefits:
- Coordinated care: Primary care providers serve as the central hub, ensuring that all care across different providers and settings is coordinated.
- Access and convenience: With extended hours and digital access, patients can reach their care team more easily and avoid unnecessary delays.
- Proactive care: Emphasis on preventive measures and continuous management of chronic conditions helps keep patients healthier and reduces the long-term cost of care.
Capitation
Capitation is a payment system where providers receive a fixed amount per patient for all their care needs during a defined period, often a month or year. This system is particularly common in managed care organizations, such as Health Maintenance Organizations (HMOs).
Mechanism:
Providers are given a set amount of money per patient, regardless of how much care the patient requires. If the cost of care exceeds the capitation payment, the provider bears the loss. However, if the cost is lower than the payment, the provider retains the difference. The fixed payment incentivizes providers to manage care efficiently, focusing on prevention and minimizing unnecessary treatments.
Key Benefits:
- Cost predictability: Both insurers and providers benefit from predictable costs, which can be budgeted more easily.
- Prevention focus: Providers are motivated to prevent illnesses and manage chronic conditions to avoid costly hospitalizations.
- Efficiency: The fixed payment system encourages providers to streamline care and deliver services as efficiently as possible.
Shared Savings Programs
Shared savings programs are designed to reward healthcare providers who can reduce the cost of care while maintaining or improving quality. Often used in ACOs, this model gives providers the opportunity to share in the savings generated by lowering healthcare expenses while still meeting performance targets.
Mechanism:
Providers participating in shared savings programs are incentivized to lower costs by improving care coordination and efficiency. If they meet quality benchmarks and reduce costs, they share in the savings with the insurer or payer. These programs aim to shift the focus from volume to value, encouraging providers to deliver higher-quality care without driving up costs.
Key Benefits:
- Incentives for efficiency: Providers are motivated to cut costs while maintaining care quality.
- Collaboration: The model encourages collaboration among healthcare providers to avoid unnecessary treatments and hospitalizations.
- Improved care outcomes: By focusing on reducing unnecessary care, providers can improve patient outcomes while lowering costs.
Maximize reimbursements with value-based billing experts
Pay-for-Performance (P4P)
What is P4P? In a Pay-for-Performance (P4P) model, healthcare providers are financially rewarded based on their performance in specific metrics. These metrics could include patient satisfaction, adherence to clinical guidelines, outcomes, and efficiency in delivering care.
Mechanism:
Providers are evaluated on how well they meet performance criteria that reflect both quality and patient experience. If they perform well, they receive bonuses or higher reimbursement rates. This model is designed to encourage providers to focus on improving care quality and patient satisfaction, rather than simply increasing the volume of services they provide.
Key Benefits:
- Quality incentives: Providers are rewarded for achieving better outcomes, improving patient satisfaction, and reducing unnecessary treatments.
- Patient-centered care: Since the model includes patient experience metrics, it encourages healthcare providers to focus on a holistic, patient-focused approach.
- Performance improvement: With financial incentives tied to performance, providers are motivated to improve their clinical practices and operational efficiencies.
Merit-based Incentive Payment System (MIPS)
The Merit-based Incentive Payment System (MIPS) is part of the Medicare Access and CHIP Reauthorization Act (MACRA), designed to streamline quality reporting for healthcare providers. MIPS evaluates healthcare providers, especially physicians, across four performance categories, influencing whether they receive bonuses or face penalties in their Medicare payments.
Mechanism:
MIPS scores providers in four key areas:
Quality: Effectiveness and appropriateness of care provided.
Cost: Efficiency in care delivery, such as reducing unnecessary treatments.
Improvement Activities: Efforts to enhance practice operations and patient care.
Promoting Interoperability: Use of electronic health records (EHRs) to improve care coordination.
Providers are evaluated on each category, with a combined score determining if they receive a positive, negative, or neutral payment adjustment.
Key Benefits:
- Encourages ongoing performance improvement.
- Clear metrics for providers to track progress.
- Providers can focus on areas that align with their strengths.
How MIPS Score is Calculated:
The MIPS score is converted into a final numerical score, typically out of 100 points. Providers who score above the set threshold (e.g., 75 or 80 points) receive an increase in their payments. Additionally, CMS scales performance to ensure that high-performing providers are rewarded with positive payment adjustments and lower performers are penalized. This scaling is used to ensure that the highest performers receive the maximum rewards.
For example:
A provider scoring 95 will likely earn a higher positive adjustment than someone who scores 75. A provider scoring 60 might face a penalty.
Alternative Payment Models (APM)
Alternative Payment Models (APMs) are an umbrella term for payment approaches that incentivize healthcare providers to deliver better care at lower costs. APMs generally provide financial rewards for meeting specific quality and cost benchmarks, and they often involve a higher level of financial risk and reward than traditional fee-for-service models.
There are two primary categories of APMs:
- Advanced APMs: These models require providers to take on both financial risk and accountability for the quality and cost of care. Examples include Accountable Care Organizations (ACOs) and Bundled Payments. Providers in advanced APMs must use certified EHRs, report on quality measures, and meet other requirements to qualify.
- Other APMs: These models may not involve as much risk, but still focus on improving care quality while controlling costs. Examples include Patient-Centered Medical Homes (PCMH) or other payment arrangements that focus on value-based care but don’t require full financial accountability.
Mechanism:
APMs reward providers for delivering high-value care, where value is defined as better outcomes at a lower cost. These models encourage coordination, quality improvement, and cost management by tying payment incentives to performance. Under APMs, healthcare organizations often assume responsibility for the care of a patient population and are reimbursed based on the quality and cost-efficiency of that care.
Key Benefits:
- Providers have an opportunity to earn higher payments by achieving better care outcomes while managing costs.
- APMs incentivize providers to focus on long-term health outcomes, rather than short-term treatments or services.
- These models emphasize the overall value of care, prioritizing preventive care, chronic disease management, and patient engagement.
Benefits of Value-Based Care Models
Value-based care models are designed to improve patient health outcomes, enhance the efficiency of resource use, and improve the financial health of providers.

- Improved Patient Outcomes: One of the core goals of value-based care is to improve patient outcomes. Providers focus on educating patients about healthy behaviors, such as better nutrition and lifestyle changes, to prevent diseases and complications. These models often require personalized care plans tailored to individual patient needs, promoting better long-term health outcomes.
- Enhanced Patient Satisfaction: Patient satisfaction improves when health outcomes such as lower mortality and complication rates, enhanced patient safety, and fewer hospital readmissions are achieved. According to the Agency for Healthcare Research and Quality, these improvements in patient care contribute directly to higher satisfaction levels.
- Reduced Healthcare Costs: Value-based care models encourage patients to engage actively in their own care, which can significantly lower healthcare costs. Research published in Health Affairs by the Robert Wood Johnson Foundation demonstrates that when patients participate actively, the costs of care are reduced. A report from Humana found that their Medicare Advantage value-based care plan saved 23.2% compared to traditional Medicare, totaling $8 billion in savings in 2022. To achieve these savings, it’s essential for providers to integrate cost data with clinical performance data to identify areas for improvement.
Challenges and Barriers to Value-Based Care
As the healthcare system shifts towards outcomes-based auto reimbursement, there are several obstacles to overcome, including financial investments, data management complexity, and regulatory challenges.
- Initial Costs and Investment: Providers in value-based care models must collect and analyze extensive data, including mortality rates, readmission statistics, procedure costs, and patient satisfaction scores. To manage this, organizations need to invest in advanced data platforms, analytics, and interoperability tools, as well as train staff to effectively use these systems.
- Complexity in Measuring Quality and Outcomes: Many healthcare organizations still face challenges with fragmented data and manual processes. To evaluate performance accurately against both internal benchmarks and industry standards, data sharing and secure storage are crucial. The National Academy of Medicine has established a framework for quality healthcare, which emphasizes the need for metrics related to effectiveness, efficiency, safety, equity, and timeliness. While metrics for safety and effectiveness are well-defined, measuring efficiency and equity remains a significant challenge.
- Resistance to Change: Health organizations often face resistance to change, particularly with the ongoing shortage of skilled professionals and high employee turnover. Providers may hesitate to shift away from traditional models of care, fearing disruption and employee dissatisfaction. However, transitioning to value-based care will require changes in clinical practices, such as focusing more on preventive care and less on managing chronic conditions.
- Regulatory and Policy Challenges: The Centers for Medicare & Medicaid Services (CMS) has introduced various value-based care pilot programs, each with specific deadlines and compliance requirements. Providers must stay on top of these deadlines, which can be time-consuming. CMS uses a combination of incentives and mandates to encourage participation in these programs, including bonus payments for demonstrating improvement in health outcomes and cost containment. The most significant deadline is in 2030, when all Medicaid and certain Medicare patients must be enrolled in value-based care initiatives. Additionally, the CMS Interoperability & Prior Authorization Final Rule of 2024, which requires improved data-sharing to reduce administrative costs and improve care, now has an extended deadline of January 1, 2027, for certain technical requirements.
Steps for a Smooth Transition to Value-Based Care Models
Making the shift to value-based care requires thoughtful planning to improve care quality, streamline revenue, and set up a foundation for long-term success.
- Focus on Preventive Care: Taking a proactive approach is key. Prioritizing measures that prevent complications, help manage chronic conditions, and reduce hospital readmissions can save costs in the long run. Regular screenings and patient education also play a big role in improving overall health and outcomes over time.
- Invest in Technology: Adopting tools like electronic health records (EHRs) and data analytics helps track patient care, spot areas for improvement, and guide better decision-making. Real-time technology is also crucial for improving accuracy and ensuring quality throughout the care process.
- Build Strong Networks: Collaboration is vital. By building partnerships between healthcare providers, care delivery becomes more coordinated. This shared effort ensures that patients receive comprehensive care, reduces fragmentation, and ultimately improves the quality of care they get.
- Engage and Educate: Training staff on value-based care principles is essential. But it’s also important to involve patients in their own care decisions. By educating both staff and patients, everyone becomes an active participant in improving outcomes, which makes the whole process more effective.
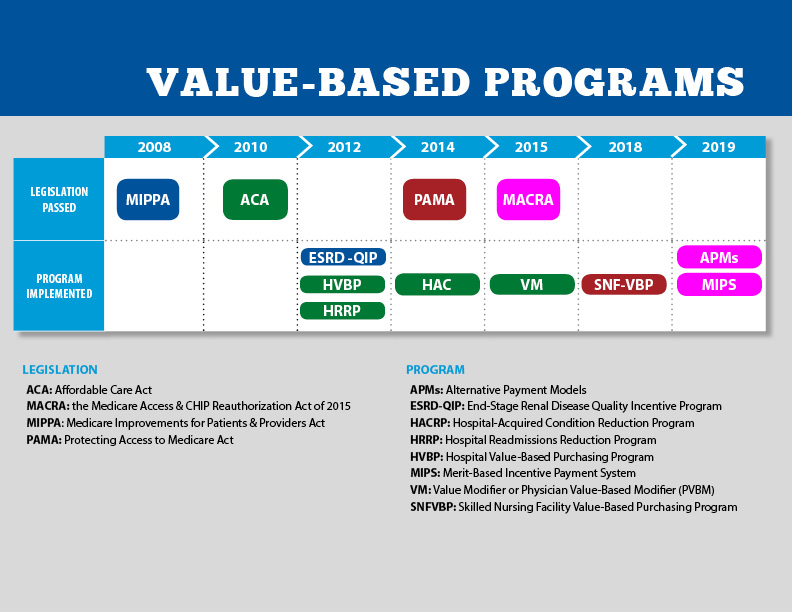
Exploring the Spectrum of Value-Based Care
CMS has piloted several health payment and service delivery models that target different health conditions and populations, including those who are underserved by traditional healthcare systems. Below are examples of some key programs:
End-Stage Renal Disease Quality Incentive Program (ESRD QIP)
CMS allocates over $153 billion annually—around 24% of its total spending—to patients with end-stage renal disease (ESRD). The ESRD Quality Incentive Program links payments to the quality of care provided at dialysis centers, aiming to improve patient outcomes by incentivizing high-quality care. Facilities that fail to meet quality benchmarks see their payments reduced.
Hospital Value-Based Purchasing (VBP) Program
This program offers incentive payments to acute care hospitals that demonstrate improvements in inpatient care across areas like mortality, complications, safety, patient experience, and infection rates. Hospitals are also evaluated on their efficiency and cost-reduction efforts. The program uses a 2% withholding from Medicare reimbursements, with hospitals that meet performance targets potentially earning back this amount or more. Starting in 2026, CMS will introduce a “health equity adjustment” to provide additional points for safety net hospitals that care for high numbers of Medicaid and disadvantaged patients.
Hospital Readmission Reduction Program (HRRP)
The HRRP aims to reduce unnecessary hospital readmissions by encouraging better discharge planning, communication, and care coordination. It penalizes hospitals that experience high readmission rates within 30 days for conditions such as heart failure, pneumonia, and chronic obstructive pulmonary disease (COPD). To manage these complex cases, pulmonary billing services are crucial in ensuring accurate coding and reimbursement for the treatment provided to patients with respiratory conditions.
Quality Payment Program (QPP)
The Quality Payment Program focuses on improving care quality and reducing costs by offering payment incentives to clinicians who meet performance standards. It has two payment models: Merit-Based Incentive Payments (MIPS), which replaced the Physician Value-Based Modifier program in 2019, and Advanced Alternative Payment Models (APMs), which target specific conditions or populations. Current APMs include models for oncology billing solutions, joint replacement, and innovations in care delivery and payment. For Physical therapy medical billing are often needed to manage the comprehensive care these patients require. (We have discussed this in detail above.)
Hospital-Acquired Condition (HAC) Reduction Program
This program reduces Medicare reimbursements to hospitals that rank in the lowest quartile for reducing hospital-acquired infections, such as pressure ulcers, post-surgical hemorrhages, and falls resulting in hip fractures. CMS also publicly posts HAC data for transparency.
Skilled Nursing Facility Value-Based Purchasing (SNFVBP) Program
The SNF VBP Program incentivizes skilled nursing facilities to reduce unplanned hospital readmissions within 30 days of discharge. Facilities are rewarded for improving care coordination and communication with hospitals to decrease avoidable readmissions. Proper nursing home medical billing plays a key role in ensuring accurate coding and reimbursement for the services that help prevent these readmissions.
Home Health Value-Based Purchasing (HHVBP) Model
Launched in 2016 by the CMS Innovation Center, the HHVBP Model aims to enhance the quality and efficiency of care provided by Medicare-certified home health agencies. It encourages the use of quality measures appropriate for home healthcare, with agencies earning incentives based on performance. In 2022, the model was expanded to include all states and US territories.
Smoothly Shift to Value-Based Care with MedCare MSO
By 2030, healthcare organizations caring for Medicare and most Medicaid patients will need to adhere to value-based care principles. Organizations should start planning now to comply with these changes. MedCare MSO’s value-based care applications are designed to support providers by offering integrated clinical, nonclinical, and unstructured data across the organization. Our services and advanced counseling solutions help healthcare providers improve care quality and control costs. We also connect care management to ensure patients receive timely, appropriate care in the right place.
Key Takeaways from the Article:
- The traditional fee-for-service model, which rewards the volume of visits, procedures, and tests, is being replaced by value-based care models that compensate providers for improving care quality and patient health outcomes.
- By 2030, the Centers for Medicare & Medicaid Services aims to have all Medicare and most Medicaid beneficiaries enrolled in value-based care programs.
- Health organizations must have a clear understanding of the costs and quality of care. Without accurate data on the costs related to patient care or disease treatment, organizations risk entering agreements that do not cover the true cost of care or provide a sufficient margin for profitability.
